|
|
||||
|
|
||||
|
|
|
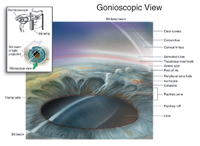
Depicting the Anterior
Eye in Two and Three Dimensions
|
| Michael O. Hughes, M.S., and Craig A. Luce, MSMI Knowledge of human eye anatomy is important to medical illustrators and ocularists. Medical illustrators are professional artists with extensive training in medicine and science who render anatomy for educational purposes. Ocularists are trained technicians skilled in the arts of fitting, shaping, and painting ocular prostheses; matching patients’ fellow (living) eyes as precisely as possible. These professions sometimes overlap, with medical illustrators becoming ocularists. Members of both professions strive to depict anterior eye anatomy with artistry and accuracy. The purpose of this paper is to describe artistic techniques of vital interest to artists engaged in depicting eye anatomy, both two and three dimensionally.
|
The visible portion of the human eye is of universal interest. This so-called “window to the soul,” figures prominently in many disciplines, from portraiture to mystical interpretation (iridology) to personal identification via computer analysis (biometrics) (Daugman, 1998). Medical illustrators and ocularists have a particular interest in accurately depicting the anterior anatomy of the eye. Medical illustrators help educate physicians and patients with depictions of anatomy that appear in articles, textbooks, and other materials. Ocularists fit and fabricate prosthetic (“artificial”) eyes. Whether for cosmesis or educational purposes, the creation of aesthetic
and accurate depictions of eye anatomy is a goal both ocularists and illustrators
share. Materials, methodology and technology challenge both professions.
However, with certain exceptions, they share a common approach: the ocularist
“paints” in three dimensions and the medical illustrator in
two dimensions. Professionally, the fields sometimes overlap, with medical
illustrators becoming ocularists.* While many medical illustrators take
courses in human anatomy and ophthalmological illustration, this article
will present information sometimes forgotten or overlooked in depicting
anterior eye anatomy in two and three dimensions. Therefore, it is the
purpose of this article to describe techniques for depicting anterior
eye anatomy in two and three dimensions. Part I of this article deals
with the cornea, pupil, and iris. All eyes depicted in illustrations are
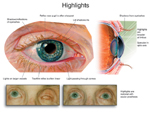
the right eye (oculus dexter or OD). For illustrators, the best way to show the more diffuse highlights on this flatter portion of the eye is to create a semi-lucent shape that fades in opacity and lightness from the source to the reflected surroundings (Figure 1). The shape of the cornea is revealed by reflections, also called reflexes,
highlights, wet-lights, or catch-lights. In the living eye, the highlights
fall in the same place on both corneas, signaling to the viewer that the
eyes are looking in the same direction. If they did not, the gaze would
appear to either diverge or converge, giving an undesirable “wall-eyed”
or cross-eyed appearance. In both life and art, highlights at the eyelid
margin reveal whether the eye is wet or dry. In ocularistry or illustration,
therefore, few or no highlights suggest a dry eye; extensive highlights
portray an eye brimming with tears. In medical illustration, highlights can be used as visual markers to
direct the viewer’s attention away from the eye itself to surrounding
details, as in illustrations of lid or facial surgery. Drawing or painting
highlights that overlap the pupil, limbus, or both will visually break
up these structures into partial circles, softening the effect of a direct
gaze. The light in such illustrations appears to be reflected from something
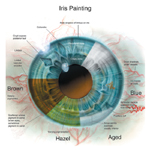
just in front of the iris (Figure 2). The Pupil Ocularists create the pupil mechanically by attaching “buttons” or “blanks” to the prosthesis. The button representing the pupil can be ground to match the pupillary diameter of the fellow eye. In addition, the ocularist may use a flat gray or brown plastic disk to represent both pupil and iris. This technique also is used when fabricating the thin, curved scleral cover shells worn over eyes that have lost vision but that remain in their sockets. Another technique requires the ocularist to simply center a pupil of thin emulsion or vinyl on the base of the iris button (Erph, 1946). The authors, representing the fields of ocularistry and medical illustration,
want to share their knowledge of anatomy and technical tips they believe
are of vital interest and importance to both professions. Members of both
professions and others engaged in depicting the human eye can achieve
excellent results by combining knowledge of anatomy, experience, observation,
and technical skills to duplicate the subtle anatomical variations in
the cornea, pupil, and other living structures. Those variations can mean
the difference between attaining, pictorically, anatomic accuracy; prosthetically,
they yield an attractive appearance or unacceptable results. For their critiques, review and encouragement, the authors thank
Howard Bartner, Chief of Medical Illustration (Ret.) at the National
Institutes of Health, Bethesda, Md; Ranice W. Crosby, Associate Professor
of Art as Applied to Medicine, Johns Hopkins University School of
Medicine, Baltimore, Md; Sara A. Kaltreider, M.D., of the Department
of Ophthalmology, University of Virginia, Charlottesville, Va; and
ocularist Joseph LeGrand of LeGrand Associates in Philadelphia, Pa.
They also wish to thank Victor Weaver (www.victorweaver.com) for graphic
design and Genevieve J. Long, Ph.D., of Portland, Ore., for writing
and editing assistance. Daugman, J. 1998. Phenotypic versus genotypic approaches to face recognition.
In Face Recognition: From Theory to Applications. Heidelberg:
Springer-Verlag.
|
Copyright 2005, The Journal of Biocommunication, All Rights Reserved